War Gaming with COVID19

The mother of all vaccines, or something like that, could start rolling out for the public-at-large in just a matter of months. This would provide relief …fingers-crossed… for years, from the personal risk of hosting this coronavirus. Yet, it will be more appropriate that the vaccine is not perceived as a personal condom to protect selected individuals from COVID19, but seen as the mainstay of a program to eradicate the virus.
There is a fine distinction between a personal prophylactic against disease and achieving population scale immunity to stop the spread of a disease. Enmasse, entire populations, or around 65 to 75 per cent as the scientists tell, must be inoculated (and in quick-time) to rid us of COVID19. The real aim of a vaccination program is to quickly and safely achieve herd immunity to halt the virus’s spread. It means coordinated vaccination at large scale and with the plan to spread the vaccine much faster than the virus can.
Just when the pandemic took centre-stage and even before the first lockdown in India, was when this article on preparing to deliver the vaccine had first mooted, that any future inoculation exercise be approached the way we address nationwide elections. For elections, many thousands of booths are set-up across the country so that not a single eligible voter is left without the opportunity; in India, the entire nation is covered in phases and within months. The COVID19 vaccination program can be conducted along similar lines – the key agenda being, to follow a predetermined timeline for complete geographical coverage, with no person left without. In this case, the result to count upon is the ousting of the viral spread.
Suppose the approach adopted is different, so as to administer the vaccine widely but to a very small category of the population (the first responders & essential workers). While these recipients will get protected, it may beget a bigger and more dangerous risk. These small number of protected individuals, scattered piecemeal amongst the rest of the population, would still come in contact with the virus and function to expose it to the effects of the vaccine… while millions of the unprotected populace still remain available as hosts. In turn, this poses the risk of triggering an aggravated sequence of mutations in this coronavirus.
This coronavirus has already mutated more than 300 times in less than a year. Reports indicate that these mutations have not undermined the vaccines under development, so far! The biggest fear is that the vaccine may prove ineffective against a future strain of the the virus. Therefore, to have a fighting chance against this pandemic, the deployment of the vaccine should be extensive and expansive. The vaccine ought to be strategically used like a weapon of mass destruction against COVID19, and not merely like a bullet proof jacket for some.
Deployment strategy
The strategy behind COVID19 eradication efforts, requires adopting tactics where the vaccine is deployed like a cluster bomb. Pick up a geography, vaccinate 65 to 70 per cent of the population post-haste, shift to the next region, repeat until the whole country is done. India could conduct this simultaneously in multiple blocks, until entire districts and states achieve herd immunity by way of vaccination. This can be achieved within weeks, like we ably demonstrate during national elections, while maintaining strict anti-covid protocols.
The protection from the vaccine will kick-in after a couple of days, and even after, those protected must not travel out into non-vaccinated regions – minimise exposing the virus to those vaccinated, where it still has other viable hosts to mutate and play its own war games. A partial vaccination program where many more unvaccinated hosts remain available to the virus, or allowing the vaccinated free travel into a viral area may lead to the failure of the new vaccine and then require another round of development.
Deployment Tactics
Vaccine coverage of 65 per cent of a population will rid it of the virus. Then, unable to find sufficient hosts to reproduce and spread, its ‘R naught’ will drop close to zero. In India, the magic ratio of 65 amounts to around 880 million people – this is not unsurmountable for India, a country that holds national elections that cater for more than 900 million voters. However, just freeing a sub-continent from the spread of COVID19 will not be sufficient, until all continents are equally free. Hopefully, the rest of the world will also pursue a mass cluster-based vaccination approach.
International effort, coordinated and inclusive, is needed so as to spread the coronavirus vaccine faster than the coronavirus.
To understand some more about administering the vaccine to a population cluster, in full and in time, let us work backwards with a few assumptions. A vaccine giver could administer a dose every five minutes and work 10 hours a day; then, s/he can inoculate 120 others every day. Two givers per vaccination site can serve 5000 people in 21 days. This example means, that Delhi with 20 million residents will require 4000 vaccination sites if the exercise is to be completed in 3 weeks. These sites cannot be the hospitals as they are still overloaded with the pandemic work load. Instead, empty movie halls, schools, malls, even local pizzerias or pharmaceutical shops can be enlisted for the purpose. Such possibilities are also discussed in another article. More the number of dispersed sites, the better, to avoid crowding… and that is still a big NO NO! Going to get a vaccine must not result in coming back with the virus.
To organise the schedule, each person in the target population can receive an appointment which they could confirm by making an online payment. If they abide with the schedule, this money (or a share) can be refunded in full. But if they ignore and crowd in before their due date, then the deposit will not be refunded. This could help coerce some discipline and prevent unplanned crowding, while easing a bit of the cash flow for the exchequer. It is here, that the high risk individuals within the target region can be allocated priority, since the entire cluster will be vaccinated in a short while in any case.
Monitoring the Deployment
The vaccine logistics system will need to monitor the vials all through their transit until it is dosed. The key aspects will be temperature-time-shock while in transit – any, exposure to inclement conditions and impact damage should be captured at each step where the vaccine exchanges custody. There are enough sensors and loggers that the blockchain can use for such record-keeping. To build in systemic checks, these ledgers could also match doses administered with the usage of syringes, swabs, any diluents, etc. A planned reverse logistics of medical waste for disposal will also benefit from such records.
Connecting the Vaccine
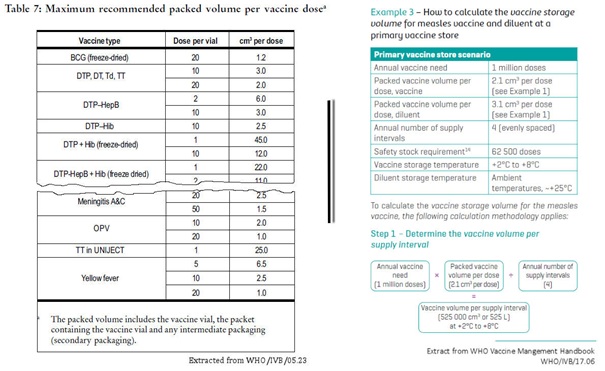
A lot of talk has surfaced, in my opinion wrongly conceived, on creating more dedicated cold stores and reefer vehicles. It will be handy to review the capacities involved. WHO has guidelines on vaccine packaging and storage, and a handbook to calculate the amount of space required for vaccines.
In the case of this vaccine let us assume that each dose is 0.5 ml and assess some of the logistics requirements. A cubic metre of space equals 1 million millilitres or can hold 2 million doses. However, the vaccine will not come in large casks but in small vials, maybe 4 doses to each and in secondary packaging. Typically, each dose of standard vaccines in will occupy a packed volume of 1.2 to 45 cm3. Obviously, this depends on whether the vaccine is dried or liquid and the number of doses per vial.
Let us continue with the loose example of 4 doses per 2 ml vial and assume each vial of the coronavirus vaccine will occupy 20 ml (twenty cubic cms) of space in the cold-chain. A twenty footer reefer container has capacity of 28 cum (60 in case of a forty footer) and it can transport 5.6 million packaged doses.
Assumption: Vaccine vial of 2 ml (with 4 x 0.5 ml doses) occupies 20 cm3 of space
• Total 4 million doses / 2 mill ml or 1 million vials of vaccine will 20 m3 of space
• A 20 feet reefer container provides 28 million cm3 of space.
• A 20 feet reefer container will hold 5.6 million doses.
• Total 1.35 billion doses will only occupy total space of 6750 cubic metres or 3,688 square metres of area if stowed up to 6 feet height.
Less than 8 such reefer containers can hold the supply of 40 million doses for all of greater Delhi. Around 250 such containers to supply 1.35 billion doses. Even if each dose is 1 ml, double the assumption of 0.5 ml, then these numbers will double. And this will not be needed all at once, but staggered to match production capacity. So, space is not a problem for bulk haulage or in storage. The situation will be different in other geographies (about 140 countries have a population of less than 20 million, with around 70 which have less than 5 million).
If the vial size and packaging is designed to suit the scale of operations, then the space can be optimised. In the current scenario, as long as daily demand is assured, the supply could actually be done in much larger doses per vial, say 50 or more. It could make the supply chain more efficient and add to overall economics – though the risk also increases. Rest assured, the complexity in first- and mid-mile logistics can be handled provided the exercise is planned well in advance. In all, the main supply and storage at vaccine depots requires very little capacity. Disposable syringes and other supplies will be the items that will actually take up more volume in transport and storage, but these should be manageable outside the cold-chain.
Last mile Distribution
The key supply chain challenge will be last-mile delivery and ensuring a vaccine holding system at each vaccination site, especially in a country the size of India. These can be passive or active cooled technologies or a combination thereof. It is here, where much detailing of implementation and planning, to match the manufacturing capacity of the vaccine, is needed. If the program is undertaken in phases to achieve cluster based coverage like during elections, the last-mile equipment could also be migrated to other locations as the activity progresses. In regions where temperatures fall below 2° Celsius, the storage space may require heating. All such plans will need to be aligned to the supply chain model, whether the vaccine supply and medical waste pickup will be every second day, or weekly, etc. The type of vaccine, temperature required and usable life are other factors. Going into further details and discussions will only lengthen this post more; and I already wonder how many even had the patience read this one, and persevere so far along.
Meanwhile, we must trust the planners who are tasked this job and ward off the virus as best we can. Until then, stay safe – stand clear of Crowds, wear a Mask, keep Clean.
PS- the above largely considers vaccine types in -20° or 2° to 8° Celsius range. The projected production data of the vaccine wanting cryogenic care, indicates their volumes primarily targets demand from North America and Europe. That -70°C vaccine will require many thousands of specialised insulate boxes with dry ice capability will be needed, from vaccine manufacturer until last-mile depots. Even then, the last-mile will come under the 2-8°C range. Luckily, such insulated boxes can also double to service the needs at each vaccination site at these higher temperature ranges.
About the author
Gubba Group: